On the 13th of May 2026, a group of occupational therapists, support workers, care providers and commissioners joined Abilia for a webinar to talk about learning disabilities, autism and technology.
Over 45 minutes, the session moved from challenge to evidence, from evidence to technology, and from technology to a real-world outcome. This article captures the key themes, the insights shared by practitioners, and what the conversation revealed about where the sector is heading.
The session's recording can be watched below. Alternatively, you can read the summary article below.
For many people living with autism or a learning disability, the gap between one activity and the next is where anxiety lives. Not knowing what comes next, or when, or in what order, is not a preference or a personality trait. It is a cognitive reality. One that shapes every hour of every day, and that touches everyone who provides support.
Understanding the conditions
Autism Spectrum Condition and learning disabilities are distinct concepts, and confusing them can lead to poor decisions, including ineffective technology choices. Recognising this difference is important not only in clinical settings but also in practical applications.
Autism is a lifelong developmental condition that affects how a person experiences the world, communicates, interacts, processes sensory information, and perceives time and sequence. It is not a learning disability. Many autistic people have average or above-average intelligence. What they often share is a profound need for predictability, structure and clear information about what is happening and when.
A learning disability is a reduced ability to learn new skills and understand complex information. It is lifelong, it ranges from mild to profound, and it typically requires ongoing support with daily living. Like autism, it is not a disease to be cured or a phase to be grown out of.
What makes both conditions particularly relevant here is that they frequently co-occur. Around one in three autistic people also has a learning disability. The overlap means that the cognitive challenges they share, around time, routine, memory, sequencing, communication and independence, are more common in combination than either condition suggests alone.
The daily challenges
Conversations with practitioners who support people with autism and learning disabilities consistently surface the same set of difficulties. These are not edge cases or exceptions. They are the everyday experience of the people being supported, and of the teams around them.
Time perception is one of the most fundamental. Not knowing how long something will take, not being able to feel the passage of time, not having a sense of how close or far away the next activity is — these are sources of genuine, sustained anxiety. For many people, the uncertainty is not occasional. It is constant.
Memory challenges compound this. Holding on to what comes next, remembering what has already been done, retaining the steps of a routine that has been followed dozens of times. All of these places demand on a system that is already stretched. The result is a reliance on other people to carry that cognitive load on behalf of the individual.
Organisational struggles, difficulty with focus and attention, low confidence in acting independently, and communication barriers that lead to frustration and friction complete the picture. None of these challenges exists in isolation. They interact, amplify each other, and together create a daily experience that is more exhausting and more dependent on external support than it needs to be.
What practitioners said
When the practitioners were asked which challenges they most commonly see in the people they support, the results were striking in their clarity.
Of 49 practitioners, 33 identified difficulty following multi-step routines and 32 identified reliance on verbal prompting from staff — the two highest responses by a clear margin.
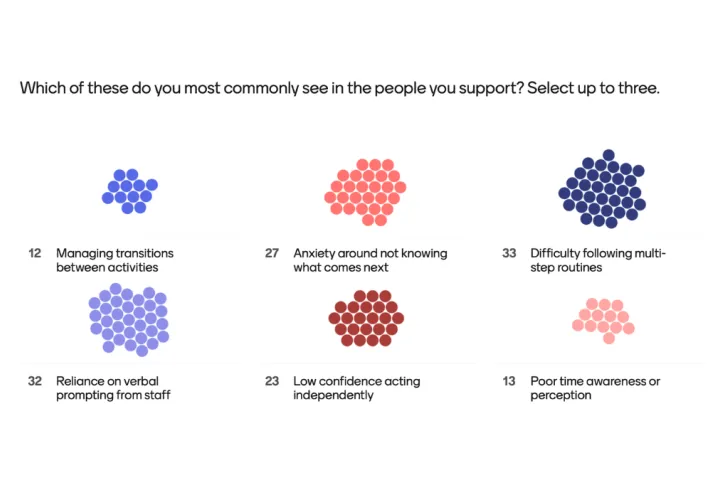
The top two responses are particularly telling. Difficulty with multi-step routines and reliance on verbal prompting are two sides of the same problem: people cannot follow complex sequences without support, and so staff become the mechanism that makes routines happen. When staff are not present, or are occupied with someone else, the individual is left without the structure they need. The technology described in the rest of this article is designed precisely to address this.
What support currently exists
The formal support for people with autism and learning disabilities is broad and, in many places, genuinely committed. From mild assistance a few hours a week to full 24-hour care, a range of provisions exists. Occupational therapists, speech and language therapists, support workers and social care teams work hard every day to help people live well and as independently as possible.
Local authorities commission services. Charities like the National Autistic Society provide guidance, advocacy and community. Educational settings are increasingly adapting their environments and approaches. For many individuals and families, this network of support is invaluable.
But the picture is under pressure. Demand is growing faster than capacity. Much of what exists still relies on human prompting — on someone being physically present to remind, to guide, to reassure, to provide the structure that the individual cannot yet generate for themselves. When that person is unavailable, the structure disappears with them.
This is where technology has a role that has been consistently underestimated in the UK, particularly for people with autism and learning disabilities. The evidence base for cognitive support technology in these populations is substantial. It is just not yet reaching everyone who could benefit from it.
The evidence behind the technology
In Sweden and Norway, cognitive support technology is not a specialist provision. It is standard care. State-funded and prescribed by occupational therapists, it is used every day by tens of thousands of people to manage their routines, their time and their independence. It sits alongside other assistive technology with the same matter-of-factness as a hearing aid or a mobility aid.
Abilia, a Swedish company, has been at the centre of this for over 30 years. The products that have become standard care in Scandinavia were not designed in isolation from the people who use them. They were co-created with individuals with lived experience, with occupational therapists who prescribe and review them, and with families and support workers who live alongside them every day.
Abilia's commitment to innovative technology for cognitive support is unwavering. Several products in the range are classified as Class 1 Medical Devices. This matters. Consumer apps and gadgets may be useful, but they are not designed, tested and regulated to a clinical standard. When a practitioner recommends an Abilia product, they are recommending something with an evidence base, a regulatory framework and a support structure behind it.
Three design principles sit at the heart of everything Abilia makes: independence, inclusion and participation. These are the criteria against which every product decision is measured. Not efficiency. Not cost reduction. Not ease of management. The starting question is always the same: what does this person need to manage their own day?
“We start with the person. What do they need to manage their day? What would it mean for them to feel in control of their time? What does independence actually look like for this individual — at home, at work, in education, in the community?”
The Quarter Hour Principle
Understanding time is different from simply reading a clock. For most people, sensing how long something will take, feeling the passage of time, and intuitively knowing whether ten minutes feels close or far are automatic processes. However, for many individuals with autism, learning disabilities, ADHD, acquired brain injuries, and other conditions that impact cognitive function, these abilities do not occur naturally.
The Quarter Hour Principle, developed by Abilia in 1993, addresses this directly. The insight behind it is simple: rather than asking someone to read a clock face, calculate a time difference and then connect that number to a feeling of duration, you show time as a visual quantity that changes as time passes.
A column of illuminated dots, each representing 15 minutes. As time passes, dots disappear. More dots means more time remaining. Fewer dots means less. When the last dot goes, the time is up. No subtraction. No clock-reading. No uncertainty about what “a bit longer” means. Just a clear, visual, immediate answer to the question “how long?”
This principle is not a gimmick. It is the foundation of Abilia’s entire range of time-support products, and it has been validated through decades of use with people who could not manage time through conventional means and now can.
Five products, one underlying need
Abilia’s cognitive support portfolio spans a range from simple and portable to fully configurable and digital. The right product for any individual is not determined by their diagnosis. It is determined by what they find difficult, what they want to be able to do, and where they are in their journey toward greater independence.
MEMO Timer
Visual countdown for transitions and waiting
A robust, waterproof, tamper-proof timer that brings the Quarter Hour Principle to its most portable form. Used in schools, workplaces, homes and community settings to support waiting, transitions, focus and self-regulation. For a young person who struggles to know when break time ends, the MEMO Timer gives them that control without requiring a single word from a member of staff.
MEMOdayboard
Whole-day visual overview for shared settings
A magnetic planning board with illuminated time pillars — red for daytime, blue for night — designed for group settings such as supported living homes, care settings and day centres. It answers the question ‘what’s happening today?’ for everyone in the room, all day, without anyone having to ask. One family introduced a MEMOdayboard for their autistic son so that when the blue lights came on, he knew it was time for sleep. The whole household benefited.
CARY Base
Personal calendar clock for daily routine
A stationary digital calendar clock that shows the time of day and the day’s activities at a glance. Personal reminders can be set, and the calendar can be updated remotely via the myAbilia web service by family members or support workers without visiting or calling. CARY Base sits between the simplicity of a visual timer and the full functionality of a digital planning system. For many people, it is exactly what they need.
HandiCalendar
Planner in your pocket — for education and employment
A smartphone and tablet app that brings the Quarter Hour Principle to the device a person already carries. Activities can be personalised with checklists, voice memos, timers and links to maps, recipes and contacts. Popular in education and employment settings because it provides structure without the distraction of other applications. For someone doing travel training, HandiCalendar can open a map to show exactly where they need to go, triggered by the activity itself.
MEMOplanner
Fully personalised digital planning system
Abilia’s flagship product and bestseller. A dedicated wall-mounted device, in Medium or Large, with a companion app, MEMOplanner Go, that mirrors the device when the user is out and about. Personalised using images and symbols rather than text, with activity checklists, a green tick completion screen, speech synthesis, video guides for complex tasks, and remote management via the myAbilia portal. The person sees their day clearly. Staff see what has been done. Family can update from anywhere.
After seeing the technology demonstrated live, practitioners were asked which product they felt could make the biggest difference for the people they support right now.
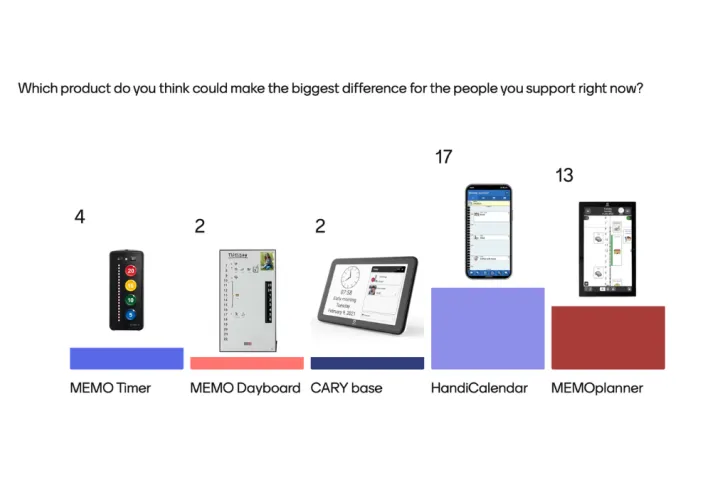
HandiCalendar 45%, MEMOplanner 34%, MEMO Timer 11%, MEMOdayboard 5%, CARY Base 5%.
The strong showing for HandiCalendar is noteworthy. It suggests that practitioners see significant potential in a solution that works on a device the person already owns and carries, particularly for those in education and employment where a smartphone is expected and a separate dedicated device might feel stigmatising. MEMOplanner’s close second reflects its status as the product with the deepest evidence base and the widest range of functionality.
Assessment in practice - the Dorset Council approach
Understanding that technology exists is one thing. Knowing how to select the right product for the right person, implement it well and measure whether it is working is another. Amanda Shelvey and Gemma Tomasso from the OT TEC Team at Dorset Council offered a practical model that any organisation could learn from.
The team — two occupational therapists, an assessment support coordinator and a principal OT, sitting within adult social care — has over 20 years of frontline community practice between them. They work across Dorset, a predominantly rural county with one of the oldest populations in England, significant digital exclusion, and long travel distances that make face-to-face contact resource-intensive. Technology is not a nice-to-have in this context. It is a necessity.
Starting with the person, not the technology
The team uses the Human Activity Assistive Technology Model as their assessment framework. The name is less important than the principle behind it: you do not start with the technology. You start with the person.
Four considerations shape every assessment. First, the person themselves: their physical ability, memory, confidence and emotional needs. What are they already good at? Where do they need support? Second, the activity: what are they trying to do? Keep safe at home, manage a routine, stay connected with others, become more independent? Third, the technology: what does it actually do? Is it genuinely easier to use, or does it create new complications? And fourth, the environment: where does the person live, who supports them, what does daily life look like, and will the technology realistically fit into it?
If any one of these four things is wrong, the whole solution can fail. A product that suits the person may not suit their environment. A product that suits the environment may not match what the person is trying to achieve. Good assessment holds all four in view simultaneously.
Outcomes, consent and ongoing review
Before any technology is introduced, the Dorset team ensures the person understands what it is, how it works and what information it may collect or share. Consent is not a formality. Where a person cannot make the decision themselves, a best interest process ensures any technology is fair, proportionate and the least restrictive option available.
When technology is provided, the work does not stop. Clear plans for use, agreed roles and responsibilities, support to build confidence with the device, and regular review to make sure the technology continues to meet the person’s needs: all of these are part of what makes implementation succeed rather than gather dust.
The team also operates a physical tech lounge — a dedicated assessment and demonstration space where people can come and try technology in a hands-on environment before any decisions are made. Not a catalogue. Not a screen. A room where someone can pick up a MEMO Timer, sit with a MEMOplanner, and experience what the technology actually feels like in daily life.
“Getting technology-enabled care right isn’t easy. It takes time, strong partnership working, and a shared commitment to do things well and not just quickly. A lot of this work starts with being open to thinking differently and having honest conversations about what might be possible, rather than defaulting to what’s always been done.”
— Gemma Tomasso, OT TEC Team, Dorset Council
What independence looks like in practice
Claudia lives with epilepsy, Addison’s disease, hypothyroidism, asthma and anxiety — the result of a brain bleed at birth. Despite these challenges, she has always wanted to live independently. That ambition is real and it matters. Technology, used well, has helped her realise it.
Before MEMOplanner was introduced, Claudia relied on prompting for much of her daily routine. The things that most people manage automatically, remembering what comes next, knowing when to start something, and keeping track of what has already been done, require someone else’s memory and presence. That dependency placed real limits on how independently she could live.
MEMOplanner changed that relationship. Activities are scheduled and personalised to her. Reminders come from the device, not from a person standing in the room. She builds her own shopping lists through the planner and uses them to do her own shopping. Her support worker, Lisa, can update the planner remotely — adding activities, adjusting plans, maintaining structure — without needing to be physically present for every interaction.
“She’s not living with her parents anymore. She’s living with her partner, a lot more independently than she was before, and it gives her control over her life.”
— Lisa, Claudia’s support worker
Claudia’s story is not exceptional. It is what happens consistently when the right technology reaches the right person through the right assessment and implementation process. The outcome: greater independence, reduced reliance on human prompting, and a life that more closely matches what the person wants for themselves, is replicable. The evidence from Scandinavia shows it has been replicated, at scale, for decades.
What the evidence points to
The challenges are real, widely experienced and well understood by the practitioners working in this space every day. The technology to address them already exists, is evidenced, regulated and in active use in real care settings producing real outcomes. The gap is not one of technology. It is one of awareness, commissioning confidence and access.
The most common challenge is difficulty following multi-step routines, which is precisely the challenge that cognitive support technology is most directly designed to address. The second most common is reliance on verbal prompting, which is exactly what technology reduces when it is implemented well. There is a very direct line between what practitioners are struggling with and what the technology offers.
The product that resonated most with practitioners after seeing the range demonstrated was HandiCalendar — the smartphone app. This matters because it suggests appetite for solutions that meet people where they already are, on devices they already carry, without requiring a separate dedicated piece of equipment. It also points toward the education and employment settings that are increasingly looking for ways to support autistic people and those with learning disabilities in work and learning contexts.
And the Dorset Council model, OT-led, person-centred, with a physical demonstration space, an outcomes framework and a commitment to ongoing review, shows what best practice looks like when an organisation decides to take technology-enabled care seriously for this population.
“It’s not experimental. It’s not complicated. And it doesn’t have to be a big leap.”
For occupational therapists, support workers, care providers and commissioners who have not yet explored cognitive support technology for the people they serve, the starting point is simpler than it might appear. See the technology. Understand what it does and who it suits. Ask the assessment questions. Start with one person, in one setting, with one clear outcome in mind.
The evidence is there. The products are here. The people who need them are already known to you.
Explore further
To request a product demonstration for your setting, explore commissioning and funding routes, or speak to the Abilia UK team about any of the products described in this article:
info@abilia.uk
abilia.uk
01954 281 210

